
In the News
What happened in healthcare recently—and what we think about it.
- H-1B visa fee struck down. The U.S. District Court for the District of Massachusetts struck down the Trump administration's $100,000 H-1B visa fee this week. U.S. Judge Leo Sorokin ruled that the administration did not have the authority to impose the fee. For now, employers can file affected H-1B petitions under the previous fee structure while the ruling remains in effect. The administration said it will appeal. Unless a higher court issues a stay, the lower fees will remain in place during the appeals process.
- The Gist: This is welcome news for healthcare organizations, some of which paused H-1B sponsorships because of the fee. The $100,000 charge created new financial and operational challenges for hospitals and health systems that rely on H-1B visa holders to meet clinical workforce needs. The ruling provides temporary relief for organizations facing persistent clinical staffing shortages, but not without uncertainty. In the meantime, hospitals and health systems that postponed H-1B sponsorship decisions because of the fee may now have an opportunity to revisit those plans while the case moves through the courts.
- Maternity care billing codes overhauled. The American Medical Association last week approved a new set of maternity care billing codes, replacing the obstetric bundled payment model with a series of codes to account for separate visits and tests. The changes were developed in collaboration with the American College of Obstetricians and Gynecologists (ACOG), which for years advocated for the overhaul. ACOG says the fee-for-service codes reflect modern obstetric care, including telehealth, home monitoring, team-based care, and individualized prenatal visit schedules. The Centers for Medicare & Medicaid Services is expected to propose reimbursement amounts for the new codes next month and finalize them in November ahead of a planned Jan. 1, 2027 implementation.
- The Gist: What gets billed gets done. This is one of the most important maternity care billing shifts in decades, signaling a restructuring in modern obstetric practice. The unbundling of codes supports more accurate reimbursement for healthcare providers and more transparent quality reporting. But concerns about the impact on patients loom large. Critics have voiced concerns that the shift from bundled payment to fee-for-service may increase out-of-pocket costs for patients. Patients with insurance pay an average of $2,743 out-of-pocket for each delivery. Critics say those with high-deductible health plans or more complex pregnancies could face additional financial strain. Hospitals may wish to prepare by reviewing the new coding guidelines and strengthening patient education efforts ahead of the transition.
- New screening guidelines for CKM. New screening guidelines were issued last week by four specialty societies to identify patients with cardiovascular-kidney-metabolic (CKM) syndrome sooner. The American Heart Association, American College of Cardiology, American Diabetes Association, and American Society of Nephrology issued the guidelines to recommend clinicians across specialties screen patients using both body mass index and waist circumference. Nearly 90% of Americans meet the criteria for CKM syndrome, according to a 2024 study. That study expands the framework of metabolic syndrome to include the diseases that emerge from it, particularly chronic kidney disease and cardiovascular disease.
- The Gist: The prevalence of CKM says it all. The screening guidelines could affect the care of most patients and the health organizations that treat them. The new guidelines encourage clinicians to see separate conditions as connected parts of the same underlying biological process—and to treat the whole patient rather than one affected organ system at a time. This reflects a new approach to risk assessment and treatment. The new framework and the screening guidelines reinforce the need for interdisciplinary collaboration and care models that enable a more integrated care approach.
Plus—what we’ve been reading.
- The hidden data trail behind health insurance exchanges. Published last month in Bloomberg, this article reports results of an investigation that found advertising and analytics trackers on state-run health insurance exchange websites used by consumers shopping for coverage. According to the investigation, some of these tools may have transmitted information about users’ healthcare interests and activities to third-party technology companies. The investigation examined state-run exchanges across the country and identified tracking technologies from major advertising and analytics companies, including Meta, Google, LinkedIn, TikTok, and Snap. While some exchanges disputed aspects of the findings or noted changes made to their websites, Bloomberg reported that several modified their tracking practices after being contacted by reporters.
- The Gist: This investigation echoes concerns raised in a recent report in The Washington Post (and noted by your faithful Gist Weekly correspondents) on companies that allegedly accessed patient records and resold them to law firms. While the circumstances differ, both stories show how health-related data moves through digital systems in ways that may not be fully understood by patients—or, in some cases, by the organizations responsible for protecting it. Which outside organizations can access patient-related information? What data are they receiving? Would patients be surprised to learn that information is being shared? Hospitals cannot address risks they cannot see. A practical first step is to inventory the vendors, platforms, and partners that receive patient-related data and evaluate whether those arrangements align with organizational policies and patient expectations. Such an arrangement can satisfy regulatory requirements and still create risk if patients would not expect their information to be shared in that way. These investigations suggest that privacy risks often emerge from the complex web of entities that touch healthcare data, not from any single technology, organization, or malicious actor.
Graphic of the Week
A key insight illustrated in infographic form.
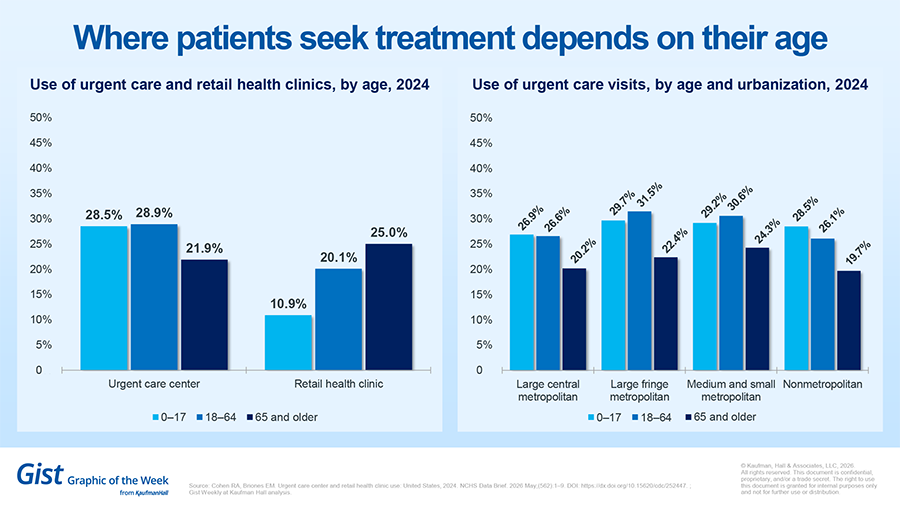
Where patients seek treatment depends on their age
Use of urgent care centers and retail health clinics varies by age, according to a report from the National Center for Health Statistics. Patients age 65 or older tended to use retail health clinics more than urgent care centers. The opposite was true for pediatric populations who visited urgent care centers almost three times as much as retail health clinics. Where patients live played only a moderate role in their preference, suggesting the importance of both options across urban and rural settings.
This Week at Kaufman Hall
What our experts are saying about key issues in healthcare.
Quality is no longer just a clinical matter. Leading hospitals should regard quality as a financial strategy. By reducing unnecessary variation and delivering more care more reliably, organizations can strengthen margins, increase throughput, and create greater strategic flexibility.
A new article explains how quality impacts operational performance, capacity, growth, and long-term financial sustainability.
On Our Podcast
The Gist Healthcare Podcast—all the headlines in healthcare policy, business, and more, in 10 minutes or less every other weekday morning.
The Gist Healthcare Podcast is on hiatus until late June. The show will return with more conversations and more healthcare business and policy news then. In the meantime, you can subscribe on Apple, Spotify, Google, or wherever podcasts are available.
Thanks for reading! The Gist is on hiatus next week. We will return June 26. In the meantime, check out our Gist Weekly archive for past editions. We also have all our recent Graphics of the Week available here.
Best regards,
The Gist Weekly team at Kaufman Hall





