
In the News
What happened in healthcare recently—and what we think about it.
- Medicaid work requirements released. The Centers for Medicare & Medicaid Services (CMS) released its interim final rule for the Medicaid Community Engagement Requirement on Monday. The rule affects Medicaid applicants and enrollees age 19 to 64 in the District of Columbia and in the 43 states and that have expanded Medicaid under the Affordable Care Act or otherwise increased access. The rule requires states to implement several requirements by Jan. 1, 2027, while additional requirements would begin a year later. Exemptions apply for certain individuals, such as those who are determined to be “medically frail;” however, exemptions may be harder to obtain as eligibility appears to be narrower than some critics expected. The interim final rule comes as states work to bolster verification systems and launch patient education efforts. Public comments on the interim final rule are accepted until July 31, the same date that the regulations go into effect.
- The Gist: Implementing the requirements will be resource intensive. The interim final rule clarifies verification requirements and deadlines, which will add administrative burden for states and can have downstream impacts for healthcare organizations. Unfortunately, states may lack the necessary infrastructure to comply, particularly as documentation requirements increase in 2028. The narrower interpretation of medical frailty may complicate matters, especially for providers. Collectively, this leaves states needing to rethink their Medicaid application platforms, renewal processes, and patient education materials quickly. Hospitals and clinicians face the prospect of patients who will need additional support to navigate the new normal and maintain documentation to stay insured.
- No Surprises Act dispute resolution process revamped. CMS and other federal departments have released a new final rule to enhance the independent dispute resolution (IDR) process of the No Surprises Act. The rule, released last Thursday, will lower administrative fees, set parameters for batching of disputes, and streamline eligibility and submission requirements. The IDR process has been overwhelmed with more than 5 million disputes, far more than the 17,000 that were initially anticipated.
- The Gist: Providers tend to win most claims, but the process is difficult and time-consuming. The new rule should help improve efficiency for CMS and providers; the changes should help providers by reducing costs and simplifying the process overall, which in turn should lead to quicker resolution. Yet some industry organizations assert that more needs to be done to eliminate misuse of the IDR process.
- The race for AI governance. The Joint Commission on Tuesday launched a voluntary certification program to provide hospitals and health systems with a framework for AI governance. The Responsible Use of AI in Healthcare focuses on organizational oversight, data management, bias mitigation, performance monitoring, and workforce education. The release comes on the heels of the Coalition for Health AI’s recent publication of implementation playbooks, which are designed to help health systems govern AI responsibly. It also comes as President Trump signed an executive order establishing a voluntary review process for advanced AI models before public release. Under President Trump’s order, technology companies may give the federal government up to 30 days to assess potential security risks associated with new AI systems. The administration also plans to establish an AI cybersecurity clearinghouse to evaluate vulnerabilities identified by advanced models.
- The Gist: AI governance is taking center stage amid growing global efforts to establish oversight frameworks. Federal AI policy and stakeholder frameworks are evolving rapidly, from broad statements of principle and voluntary guidance toward more formal governance structures. And everyone wants a say. For U.S. hospitals, this signals a shift toward greater accountability for how AI is selected, implemented, monitored, and managed. Healthcare organizations will ultimately be expected to demonstrate not only that AI delivers value, but also that it is deployed safely and responsibly, and with appropriate safeguards to maintain patient trust.
Plus—what we’ve been reading.
- Jet-setting travel nurses. A recent The Wall Street Journal article profiles travel nurses whose jet-setting career path following the Covid-19 pandemic garnered social media attention. Nurses describe trading traditional staff roles for temporary assignments that offered higher pay and the chance to explore new places. Nurses boast of much higher wages and a lifestyle that enables experiences like skydiving in Hawaii or exploring jazz clubs in Chicago. Not all work locations are glamorous, of course, and the work remains defined by uncertainty, including contract instability, housing challenges, benefit disruptions, and social isolation.
- The Gist: This lifestyle may sound alluring to nurses, but travel nursing is also an expensive line item for hospitals, which must manage volatility, seasonal demand, leave coverage, and workforce shortages. While travel nurse usage has been scaled back since the pandemic, hospitals continue to rely on them for staffing flexibility, while nurses value greater autonomy. But the model continues to strain hospital budgets and sometimes creates tension among clinical teams over pay disparities. The sustained demand for and interest in travel nursing indicates a workforce challenge that is likely to persist in an uncertain labor market.
Graphic of the Week
A key insight illustrated in infographic form.
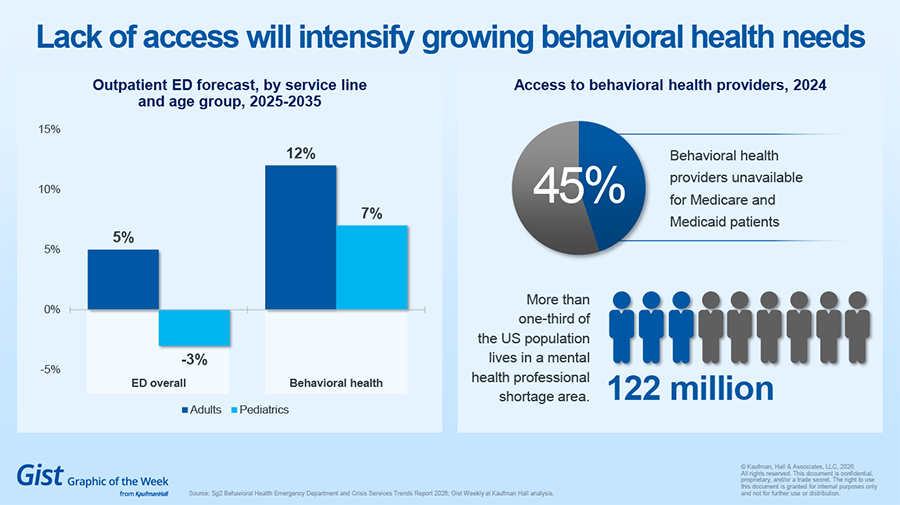
Lack of access will intensify behavioral health needs
The latest Sg2 outpatient ED forecast shows behavioral health ED visits will grow faster than overall ED visits over the next decade. Behavioral health patients often stay in the ED longer, which can slow throughput and increase wait times. Workforce constraints will only add to the pressure. Approximately 40% of the U.S. population lives in a federally designated Mental Health Professional Shortage Area, with rural counties being more likely than urban counties to lack behavioral health providers. Meanwhile, nearly half of behavioral health providers are unable to take on additional Medicare or Medicaid patients.
This Week at Kaufman Hall
What our experts are saying about key issues in healthcare.
Hospital rankings were designed to improve transparency and help patients make informed decisions. Today, they influence far more than consumer choice.
Public scorecards shape reputation, recruitment, payer negotiations, strategic priorities and investment decisions. Yet healthcare leaders increasingly question whether the growing focus on rankings is driving meaningful improvement or pulling resources away from patient care.
A new article examines the growing debate around hospital rankings, the operational burden of participation and what leaders should consider when evaluating the value of public scorecards.
On Our Podcast
The Gist Healthcare Podcast—all the headlines in healthcare policy, business and more, in 10 minutes or less every other weekday morning.
The Gist Healthcare Podcast is on hiatus until late June. The show will return with more conversations and more healthcare business and policy news then. In the meantime, you can subscribe on Apple, Spotify, Google, or wherever podcasts are available.
Thanks for reading! We’ll see you next Friday with a new edition. In the meantime, check out our Gist Weekly archive for past editions. We also have all our recent Graphics of the Week available here.
Best regards,
The Gist Weekly team at Kaufman Hall





