
In the News
The biggest news of the week—and what we think about it.
- Court orders Leapfrog Group to remove safety grades. A federal judge in Florida last Friday ordered The Leapfrog Group to remove safety grades it assigned to five hospitals, ruling that the ratings were “deceptive and unfair.” The decision stems from a lawsuit filed by Tenet Healthcare in its Palm Beach Health Network after the five hospitals received low grades in Leapfrog’s 2024 and 2025 reports. Tenet argued that Leapfrog operated a “brazen pay-to-play scheme” through its “memberships,” in effect pushing hospitals to participate in its surveys. U.S. District Judge Donald Middlebrooks found that Leapfrog’s methodology penalized hospitals that did not participate in its voluntary survey by assigning them artificially low scores using “imputed” or assumed data. Leapfrog said it will comply with the order but plans to appeal, arguing the ruling threatens the ability of ratings organizations to publish evaluations.
- The Gist: The ruling touches a long-running tension with private ratings groups that wield significant influence over reputation. When it appeared on the scene 25 years ago, The Leapfrog Group was a true pioneer in the national patient safety and quality agenda; but some hospitals chafed at its public reporting requirements. Safety ratings are widely used by employers, health plans and consumers to compare hospitals, yet the data sometimes rely on voluntary reporting or statistical assumptions when information is missing. In this case, the court concluded that assigning failing scores to hospitals that declined to submit data could mislead the public about actual patient safety. The case illustrates the real financial and reputational stakes attached to these rankings. The decision could embolden hospitals to challenge rating methodologies they believe are flawed or punitive; yet limiting an agency’s ability to publish ratings could weaken transparency efforts aimed at helping patients assess hospital quality.
- Non-network plans proposed for ACA. The Trump administration last month proposed a rule introducing the prospect of health plans without a list of in-network doctors and hospitals for Affordable Care Act (ACA) patients. Under these “non-network” health plans, insurers would set a fixed payment for each service, and patients would shop for providers who would accept that amount. The plans, which would be made available on ACA health insurance exchanges next year, would shift responsibility to consumers to compare and negotiate prices and bear the cost of any price difference. These plans may cost less for patients, especially after the expiration of the ACA enhanced premium tax credits, and may reduce costs. States would have the ultimate decision to allow the sale of these plans, and insurers would have to prove that at least some providers would accept payments as sufficient.
- The Gist: Non-network plans aren’t exactly new—for instance, such plans were sold in Wisconsin back in 2016. If these lower-premium plans make it to the exchanges, they could be an opportunity to keep prices down for consumers. Advocates say they also engage patients as active participants in their care, but they could present significant cost exposure to patients who may be left footing the bill if there is a difference between what providers charge and what plans will pay. Non-network plans appear to be the latest attempt to curb costs and rebalance who carries and negotiates financial risk, much as catastrophic and high-deductible plans before them. For hospitals, the growth of non-network plans could ultimately translate to more underinsured patients—and potentially more bad debt.
- Healthcare jobs drop following strikes. The healthcare field lost 28,000 jobs last month, according to a Bureau of Labor Statistics report published last Friday. This comprised a significant portion of the total of 92,000 jobs lost in February. Hospitals added 12,000 jobs, but physicians’ offices lost 37,000 jobs, primarily due to massive, since-resolved healthcare strikes in New York City and in California and Hawaii, the agency said. The new job losses come after a strong January in which the healthcare field grew by 77,000 jobs, and an average of 36,000 jobs added monthly over the past year.
- The Gist: Healthcare has long been viewed as the engine of the U.S. economy. Last month’s healthcare job decline comes after consistent growth. After a year of steady hiring in healthcare, the blip may very well be a temporary impact of the recent strikes. The healthcare labor market should bounce back, driven by an aging population with medically complex needs, even as the overall U.S. job outlook remains sluggish. Bouncing back and maintaining a thriving healthcare workforce will likely need investments in staff retention, workforce pipelines and innovative workforce models.
And—and what we’re following.
- Medicare premiums were 10% higher last year because of potential overpayments to Medicare Advantage plans, according to the Joint Economic Committee, a bipartisan group of congressional lawmakers, in findings released Tuesday.
- The cybersecurity monitoring advisory group Health Information Sharing and Analysis Center last week warned U.S. health organizations of the potential for cyberattacks from state-sponsored or loosely aligned “hacktivists” as retaliation for U.S. military strikes on Iran.
Plus—what we’ve been reading.
- Rebuilding trust demands candor. Published late last month in HealthLeaders, this article features an interview with healthcare executive Sachin Jain, M.D., CEO of SCAN Health Plan, who argues that healthcare suffers an essential failure: a culture of “quiet complicity.” In the interview, which follows a commentary he wrote in Forbes outlining 10 leadership resolutions, Dr. Jain describes how leaders privately agree that hard truths exist, yet they remain publicly silent about them. This, he says, reinforces “a broken status quo.” Dr. Jain criticizes what he calls “toxic positivity” that masks friction, and warns that mission-driven rhetoric feels limited, often diverging from patient experience. Rebuilding trust, he contends, requires candor about shortcomings, structural change in incentives and visible accountability rather than branding campaigns that leave patients “gaslit” about their experience.
- The Gist: Dr. Jain argues that trust will not be rebuilt through messaging alone. His biting critique carries weight because he works within the system he challenges, calling out his own community. When healthcare organizations use scripted responses, opaque processes or brand language that smooth over friction, they risk deepening the disconnect rather than bridging it. If honesty feels uncomfortable, that is the point; rebuilding trust demands willingness to lead with honesty, values and recognition of shared humanity.
Graphic of the Week
A key insight illustrated in infographic form.
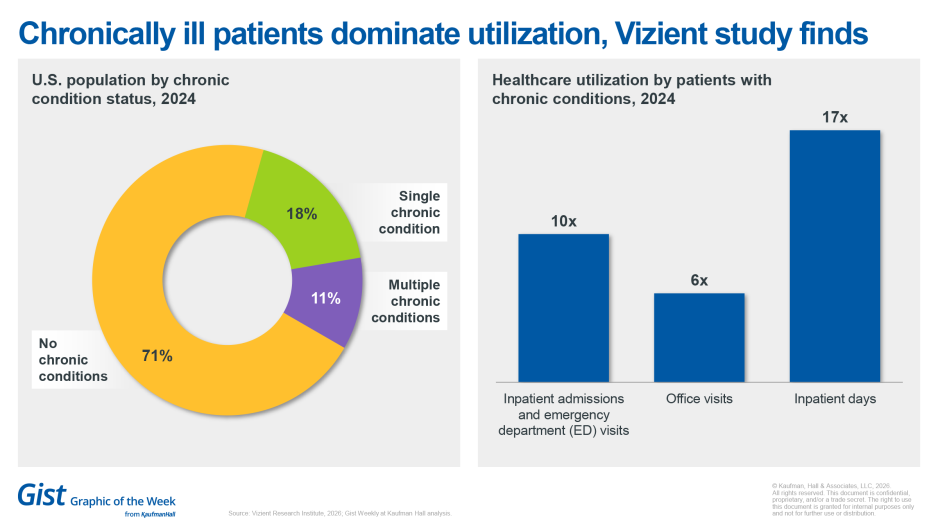
Chronically ill patients dominate utilization, Vizient study finds
The latest Vizient Research Institute study, The access imperative: Reimagining care delivery for a more complex patient population, concludes that the bulk of hospitalizations in the United States are due to chronic illness. Patients with chronic conditions generate roughly 10 times more inpatient admissions and emergency department visits and more than six times as many office visits compared with those without chronic care needs. On a per capita basis, they generate about 17 times more inpatient days. With more than 80% of hospitalizations involving Americans with at least one chronic condition, chronic care drives most of the healthcare utilization. The findings underscore that healthcare leaders cannot afford siloed care, and the future belongs to organizations that strategically prioritize integrated chronic care models to meet rising demand and manage complexity.
This week at Kaufman Hall
What our experts are saying about key issues in healthcare.
Following a period defined by operational strain, workforce disruption and financial pressure, healthcare leaders are now turning their focus toward technologies that can help rebuild stability as they prepare for the future. Artificial intelligence (AI) is a central point of exploration for health systems seeking greater efficiency, improved patient experience and sustainable clinical operations.
During a recent executive dialogue hosted by the American Hospital Association, healthcare leaders explored the practical realities of AI adoption on topics including governance, workforce expectations, vendor strategy and how best to measure value in a rapidly evolving technology environment.
On our Podcast
The Gist Healthcare Podcast—all the headlines in healthcare policy, business and more, in 10 minutes or less every other weekday morning.
Earlier this week, we heard the second half of host J. Carlisle Larsen's conversation with Kaufman Hall Managing Director Joyjit Choudhury about how health systems can prepare for a future in which site-neutral payments are a common part of the healthcare reimbursement landscape. (You can find the first part of their conversation here.)
Coming up this Monday, JC is joined by Modern Healthcare’s Michael McAuliff to get the latest in how healthcare policy is shaping up on Capitol Hill, and how healthcare could play a role in the upcoming midterm election.
To stay up to date, be sure to tune in every Monday, Wednesday and Friday morning. Subscribe on Apple, Spotify, Google or wherever podcasts are available.
Thank you for reading! Please stay tuned for next week and check out our Gist Weekly archive for past editions. We also have our recent Graphics of the Week available here.
The Gist Weekly team at Kaufman Hall





