
IN THE NEWS
What happened in healthcare recently—and what we think about it.
- Trump budget request includes healthcare cuts. President Trump last Friday released his FY2027 budget request, outlining significant healthcare spending cuts. The budget would include a 5% reduction to the Department of Health and Human Services from the FY2026 enacted level. It includes cuts to National Institutes of Health (NIH), the Agency for Healthcare Research and Quality, and the Administration for Strategic Preparedness and Response. Like last year, the administration proposed a new entity, Administration for a Healthy America, under which it would consolidate several current operating divisions. The budget request includes proposals to eliminate NIH’s National Institute on Minority Health and Health Disparities, the National Center for Complementary and Integrative Health, and the Low-Income Home Energy Assistance Program (LIHEAP).
- The Gist: The budget request, like all presidential budgets, is an outline of the president’s priorities, but not binding policies. It reflects the administration’s continued efforts to reform federal healthcare operations and spending. The proposed elimination of programs tied to social support, public health infrastructure, and global engagement underscores the direction the administration wants to go. It includes an explicit effort to reduce waste and redundancy, but cuts to health research funding, if enacted by Congress, would pose significant challenges for academic medical centers. The elimination of programs such as LIHEAP may place additional strain on hospitals, potentially driving higher demand tied to unmet social needs. Because it carries the imprimatur of the White House, the proposal carries weight; but it is Congress that ultimately controls the purse strings and sets the budget.
- Stricter vetting slows physician pipeline. Earlier this year, the Trump administration expanded immigration screening rules affecting foreign physicians, with U.S. Citizenship and Immigration Services (USCIS) late last month outlining an update that intensifies vetting of foreign nationals seeking visas and immigration benefits. The agency called prior screening processes “wholly inadequate” and is now applying stricter measures, including enhanced background checks and biometrics. The guidelines build on executive actions restricting entry from 39 countries and requiring more rigorous application review. The new posture is already having effect, as visa processing for foreign physicians has slowed sharply, leaving some physicians unable to work despite approved roles in U.S. hospitals.
- The Gist: The policy direction means immigration enforcement goals are directly colliding with workforce realities in healthcare. Delays and additional scrutiny have an outsized effect on doctors serving in rural and underserved areas already facing staffing shortages. International medical graduates account for roughly one-quarter of U.S. physicians, who rely on visa renewals (e.g., H-1B, J-1), green cards, and work authorization to practice. These physicians fill a significant share of residency and fellowship positions and around half serve in rural and underserved communities; roughly 60% practice in primary care fields; and thousands of doctors could be affected. This might show up as canceled clinics, longer wait times, and reduced access to care at the local level. A tighter front door for immigration appears to make a narrower pipeline for care delivery, and hospitals may already be feeling the impact.
- Insurers claim progress on prior authorization. Health plans say they are making progress on prior authorization in a new industry report released this week. The report, from the health insurance trade group AHIP and the Blue Cross Blue Shield Association, surveyed health plans and found an 11% reduction in prior authorization requests, new 90-day continuity-of-care protections, and improved communication around denials and appeals. The update comes as part of a voluntary pledge by insurers to reduce administrative friction and improve the patient experience. Plans also reiterated a longer-term goal to move toward electronic workflows and near real-time prior authorization decisions by 2027.
- The Gist: The AHIP report follows sustained regulatory and political pressure to reform prior authorization practices, which have grown increasingly unpopular. Health plans frame the changes as a meaningful step toward simplification and reduced burden; but for hospitals, the practical impact remains limited. An 11% reduction still leaves the vast majority of prior authorization requirements in place, and there is little visibility into whether high-friction services were meaningfully affected. Most of the operational pain points, such as manual processes and payer variation, remain unchanged in the near term. While nearly two-thirds of providers surveyed by Aetna agree that prior authorization has a legitimate role to play, less than half say payers prioritize patient wellbeing and clear information. Because the commitments are voluntary, consistency across payers is far from guaranteed. The net effect is incremental improvement, not a structural shift in how prior authorization affects patients or hospital operations.
Plus—what we’ve been reading.
- Behind the Alzheimer’s diagnosis controversy. Published in February in The Wall Street Journal, this article delves into the frustrating science behind Alzheimer’s disease. Doctors still cannot agree on how to diagnose the disease, and the disagreement is based on definition. Competing frameworks define the disease either by biology, such as amyloid plaques in the brain, or by the presence of cognitive symptoms. This can lead to inconsistent diagnoses for the same patient. Some clinicians argue that early detection based on biomarkers enables earlier intervention, but others warn that these markers are common in older adults who may never develop dementia. New blood tests and imaging tools are making screening easier, making the lack of consensus around what constitutes Alzheimer’s more visible, and more consequential.
- The Gist: Few diagnoses carry as much gravity to patients and their families as Alzheimer’s. Misdiagnosis can expose patients to unnecessary treatments, including drugs with known risks, and create significant psychological harm. This lack of consensus is an operational problem waiting to happen. Inconsistent definitions complicate care pathways, utilization management, and eligibility for high-cost therapies, particularly as demand for testing rises. The risk of overdiagnosis introduces downstream costs, while underdiagnosis carries its own quality and liability concerns. Health systems will want clearer governance around when to test, how to interpret results, and who qualifies for treatment. Just as important, hospitals will need to manage patient expectations as screening expands faster than the evidence base; the science may still be evolving, requiring health systems to balance clinical rigor with the realities of patient demand.
Graphic of the Week
A key insight illustrated in infographic form.
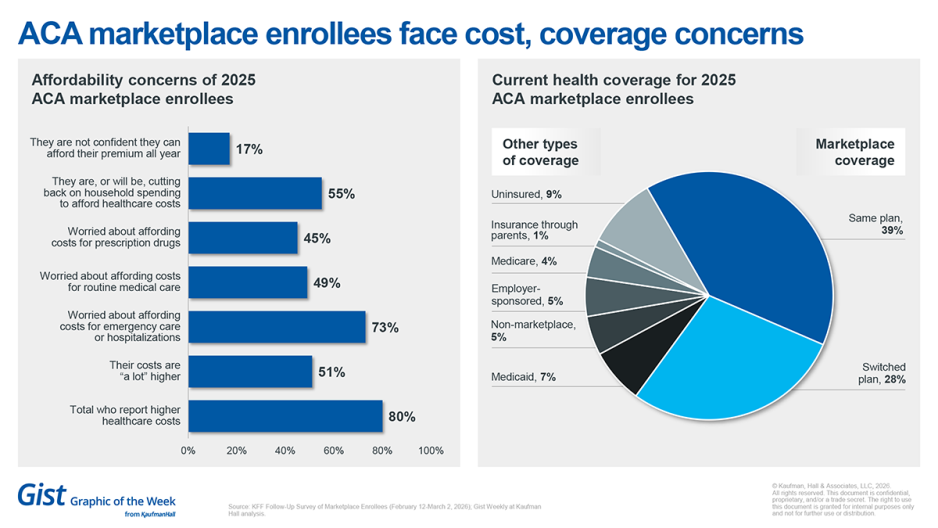
Costs spike, coverage slips in ACA marketplace
A recent KFF follow-up survey shows the reality of the expiration of Affordable Care Act (ACA) enhanced tax credits is hitting consumers hard: 80% of ACA marketplace enrollees report higher healthcare costs, with 51% saying those costs are “a lot higher.” The financial strain is tangible, as 55% say they are cutting back on household spending to afford coverage and 17% are not confident they can pay premiums all year. Coverage is also shifting, with 69% remaining in marketplace plans but 28% switching plans and 9% now uninsured, largely driven by cost pressures rather than changes in health needs. These data point to a market under stress, in which rising costs are reshaping both consumer behavior and coverage stability.
This Week at Kaufman Hall
What our experts are saying about key issues in healthcare.
Hospital and health system M&A activity strengthened in Q1 2026 with 22 hospital and health system transactions announced—the highest Q1 activity since 2020. The robust activity this quarter continues a steady recovery in M&A activity that began in the second half of 2025. Read the full analysis in our Q1 2026 M&A Activity Report.
On Our Podcast
The Gist Healthcare Podcast—all the headlines in healthcare policy, business and more, in 10 minutes or less every other weekday morning.
Earlier this week, we revisited JC’s conversation with Kaufman Hall’s Bonnie Proulx on why many health systems aren’t seeing a payoff when they hire more advanced practice providers, and how leaders can rethink their physician–APP models.
This Monday, JC speaks with Dr. Robert Wachter, Chair of the Department of Medicine at the University of California, San Francisco, about the latest wave of AI in healthcare, and whether it represents a real turning point or another familiar cycle. In Part 1 of a three-part series, they look at what feels genuinely different about this moment, and what lessons from the rollout of electronic health records still apply.
To stay up to date, be sure to tune in every Monday, Wednesday, and Friday morning. Subscribe on Apple, Spotify, Google, or wherever podcasts are available.
Thanks for reading! We’ll see you next Friday with a new edition. In the meantime, check out our Gist Weekly archive for past editions. We also have all our recent Graphics of the Week available here.
Best regards,
The Gist Weekly





