Service line dashboards that actually drive strategy and action
Health system service lines have no shortage of data, capable of producing dozens of charts in an instant. Most leaders review disparate spreadsheets constantly to assess when performance is off track. The problem is understanding what comes next.
Data alone are failing to answer the right questions at the right time in the right way. Many organizations cannot agree on which decisions the service line must make, so they cannot clearly define what the data should inform. As a result, organizations report and track performance but often do not use the data to guide action.
Consider it a great paradox of modern service line management: we have more data than ever, yet less clarity about what to do with these data.
Many organizations have considered connecting data assets through a dashboard. This is a smart approach—but it must be managed with care and precision, because a dashboard cannot in and of itself point an organization in the right direction. A dashboard might be too cold (that is, sparse and missing important signals), or too hot (crammed with metrics, flashing alerts, and endless drill-downs that obscure more than they reveal).
The effective dashboard splits the difference. It surfaces a few measures that drive performance, provides enough context to act, and filters out the noise. This is why the best service line dashboards are illuminating but parsimonious: they tell the organization everything it needs to know, but do not overwhelm with extraneous data.
Why service line dashboards are different
Traditional dashboards work in environments with clear ownership and span of control. An emergency department leader can see a metric, assign accountability, and drive change within a defined team.
But service lines operate differently than traditional departments, so their dashboards should work differently too. At their best, service lines coordinate clinical care at scale, align physicians and the health system, and manage performance across the continuum. This is why they have re-emerged as a primary operating structure and strategic engine for many organizations. They span multiple settings and rely on physicians who may not share the same incentives or reporting structure. Performance reflects coordination across the continuum, not a single unit.
There is a lot at stake. This heavy lift demands analytics that support leadership, strategy development, stakeholder alignment, market dynamics, and care coordination. Thus, a dashboard that works for a department might break down in a service line. A traditional dashboard may show variation in care or outcomes but might not reveal where that variation originates or how to correct it. A service line’s inherent complexity requires analytics that help leaders navigate across settings and stakeholders.
Unfortunately, many service line dashboards are built in isolation from these foundational attributes. They often remain heavily weighted toward activity metrics such as volume trends, market share, publicly reported quality measures, and cost per case. Financial metrics are sometimes present, though usually without sufficient integration into strategic context. Far less common is explicit agreement on the handful of questions the service line must answer and alignment between those questions and the metrics used to track performance.
This ambiguity often reflects an unresolved governance issue. Organizations vary in whether service line strategy is set at the enterprise level or developed locally. The scope of authority can be equally uneven; in some systems, service lines are responsible for strategic planning, growth, key performance indicator tracking, and quality improvement; in others, physician recruitment, budgeting, and ambulatory strategy remain fragmented across departments and markets.
Most systems also push standardized dashboards from the enterprise level. While this enables consistency, it often leaves little room for service line leaders to tailor metrics to their own initiatives or specific needs.
Stop arguing about the data
It is common, when dashboards surface uncomfortable realities, to question the numbers. Definitions are scrutinized and new iterations are commissioned. When dashboards fail to point to a clear course of action, debating the data becomes the path of least resistance.
While methodological rigor is appropriate, the pursuit of perfect data can become an excuse to defer difficult decisions. Most transformative actions do not require flawless measurement. Rather, they require directional clarity and predefined thresholds that trigger intervention. A concise, agreed-upon set of measures, defined in advance and tied to decision pathways, is more powerful than an exhaustive catalog that diffuses accountability.
Analytics matter more when existing in support of the key priorities, strategies, or goals set by a service line. They should also be purpose built to align with:
- A clear leadership structure, often built around the physician–administrator dyad, that depends on shared data to connect clinical credibility with financial discipline
- A coherent strategy, whether enterprise-led or locally shaped, grounded in metrics that show how service line decisions advance broader goals
- Stakeholder alignment across employed and independent physicians, across markets and across care settings, sustained by consistent definitions and transparent reporting
- Strong system-of-care coordination, which requires analytics that link inpatient and ambulatory strategy, referral patterns, access and quality into a single view.
- The ability to translate performance signals into specific actions across sites, settings and stakeholders.
Before commissioning another dashboard, health system leaders should examine what they already have. Does it fully capture questions about the costs of deploying the service line? Does it clarify the relationship among volume, quality, contribution margin, and market position? Does it point to where capital and talent should be? When a metric crosses a threshold, is a specific decision triggered? When a metric turns red, does the dashboard indicate where the problem is occurring and who owns it?
Figure 1. An illustrative example of a dashboard
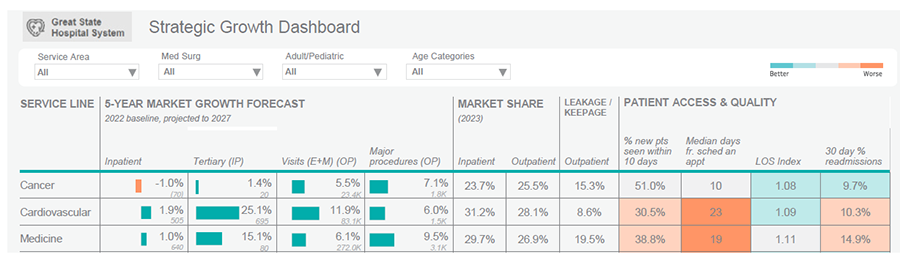
Service line dashboards: what to look for
Organizations should design dashboards to integrate performance across hospitals, clinics, ambulatory surgery centers, and physician practices rather than forcing leaders to assemble fragmented reports independently. Service line leaders need a unified view of performance across the continuum, including operational, clinical, and financial measures that can be interpreted together rather than in isolation.
Dashboards should identify the drivers of variation, not merely display variation itself. When performance deviates from target, leaders should be able to determine where the problem originates and what response is required. By connecting performance signals directly to decisions and ownership, the ideal dashboard accelerates accountability.
Organizations should also establish different review cadences for different metrics. Some indicators require weekly intervention and rapid escalation, while others are better suited to quarterly strategic review. Treating every measure with equal urgency obscures priorities and creates unnecessary noise. Effective dashboards distinguish between operational monitoring and strategic oversight.
Health systems should minimize reliance on manual data entry whenever possible. Dashboards that depend heavily on manual inputs are more vulnerable to error and inconsistency. Automated, standardized data pipelines improve confidence in the numbers and reduce delays in decision-making.
Some organizations are beginning to incorporate advanced analytics. These identify patterns as they emerge and direct leaders toward areas requiring intervention. Used appropriately, these tools can reduce the analytic burden placed on service line leaders and support faster, more targeted action.
In high-performing service lines, dashboards are concise and tied explicitly to enterprise priorities. They present a limited set of measures linked to growth, access, quality, margin, and physician alignment, with clear targets and interim milestones. They provide enough context to identify where problems originate and what action should follow. In some organizations, dashboards are supplemented with brief narrative interpretation to clarify emerging risks and strategic implications.
If the dashboard cannot support faster, clearer decision-making, it is not functioning as a strategic tool. It is just a reporting exercise. Dashboards become instruments of intent only when they are designed to force choices about growth and resource allocation. Anything less may appear sophisticated, but it will not alter the trajectory of the enterprise.
Five essential enterprise questions a service line dashboard should answerA service line dashboard should not merely describe performance. It should answer these strategic questions that shape enterprise action:
If a dashboard cannot answer these questions clearly and consistently, it is unlikely to influence capital allocation, recruitment strategy, or portfolio design.
|
The service line dashboard self-auditA service line dashboard should carry decision-linked thresholds, not just activity metrics.
|
When you’ve seen one dashboard… you’ve seen one dashboardIf you’re looking for a model dashboard, stop. There is no universal service line dashboard. Different service lines may require different metrics depending on their strategic priorities and underlying drivers of performance. Any template that claims to be “best practice” without reference to strategy is, at best, incomplete. Dashboards are not off-the-shelf products. They are instruments built to answer specific enterprise questions. For instance, an organization investing heavily in physician alignment will require deeper visibility into deployment costs and contribution margin than one operating in a mature employed model. Of course, data should be standardized to enable benchmarking. But the right dashboard begins with a mandate: what decisions must be made about scale, consolidation, recruitment or capital allocation? What tradeoffs are leadership prepared to confront?
|

Intelligence