


Since the introduction of the Centers for Medicare & Medicaid Services’ two-midnight rule for determining observation status in 2013, observation patients have represented a growing percentage of hospitals’ daily censuses. Although the CMS rule technically applies only to traditional Medicare beneficiaries, similar methods for determining observation status have been adopted by commercial health plans.
We know the percentage of observation status patients has grown; what we have not been able to do is determine what might be an appropriate percentage of observation status patients. Starting in February 2022, Kaufman Hall’s National Hospital Flash Report began publishing a new metric that will track the number of observation patient days as a percentage of total days across the more than 900 hospitals that currently contribute data for the report.
While determining observation status is and should be a decision driven by physician judgment—and the percentage of patients in observation status will vary from hospital to hospital—this new metric will help management understand how much their observation status percentages vary from the median. If that variance is significant, management can investigate and, if appropriate, address the factors or processes that are driving the variance.
The importance of appropriate status assignment
Getting observation status right is important to patients, their providers, and the organization:
- For patients, observation status can mean higher copays and—if they need to be discharged to a skilled nursing facility—Medicare coverage of their post-discharge care may be affected.
- For providers, who have a regulatory requirement to inform patients of their observation status and its implications, observation status can create tension within the patient/provider relationship due to reimbursement or copay implications.
- For hospitals, observation status assignment means a lower payment rate for the care the patient receives. Patients who are inappropriately assigned observation status can also tie up beds in the emergency department or on inpatient units, which can slow patient throughput, interfere with efficient delivery of services, or suggest the need for additional capacity—and the significant capital expenditures that come with it—even if that need may not in fact exist.
These are the downsides to observation status, but if managed well and in compliance with CMS guidelines and other payers’ contractual terms, these negative aspects can be minimized.
Under CMS guidelines, observation status should be applied to a well-defined set of specific, clinically appropriate services, including short-term treatments, or when additional time is required to determine whether a patient will need further treatment on an inpatient basis or can be safely discharged from the hospital. If a physician expects that the patient will need a hospital stay crossing two midnights and the medical record supports that expectation, observation status will typically not be appropriate. Even if the stay will be less than two midnights, if the service the patient is to receive is on CMS’s “inpatient only list” or the physician expects that the patient will require inpatient services, observation status again would typically not be appropriate.
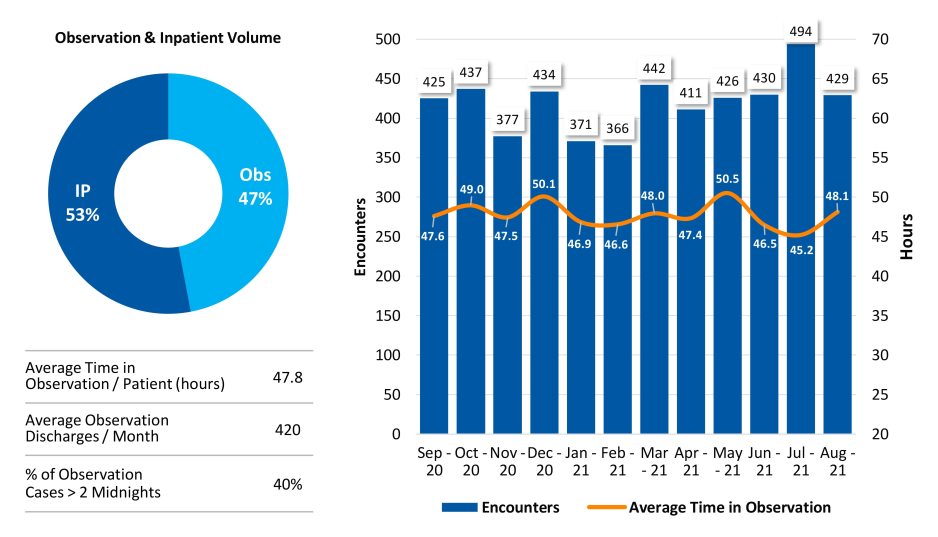
If observation status is being appropriately assigned, few observation patients should have a LOS exceeding two midnights. If a significant percentage of observation patients have stays exceeding the two-midnight benchmark, inappropriate assignment may be an issue. Figure 1, for example, shows data for a hospital at which 47% of the discharges are observation, with 40% of the observation patient stays exceeding two midnights and an average LOS of just under 48 hours. These data suggest that too many patients are being assigned to observation status or that the process for timely discharge of observation patients is flawed, and that further investigation is warranted.
Figure 1: Analysis of Observation Patient Status and Length of Stay
Tactics to ensure appropriate assignment
There are several tactics that management and clinical leaders can deploy to ensure that the status is being assigned appropriately.
Protocols. Clearly defined protocols for assigning observation status generally—and for determining the appropriateness of observation for conditions where the status is frequently assigned (e.g., atrial fibrillation, chest pain, congestive heart failure, chronic obstructive pulmonary disease, and syncope)—establish clear criteria to support individual physician decision-making. These criteria also provide the detail necessary in the medical record if an assignment to inpatient status is challenged by a payer. If a patient’s status changes, the protocols also help determine when reassignment to inpatient status is appropriate.
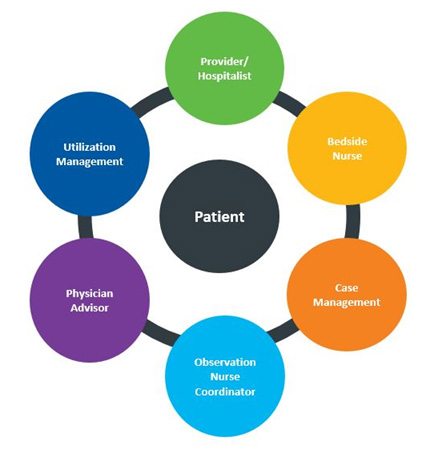
Observation care management teams. A dedicated, multidisciplinary observation care management team (OCMT) can improve care delivery and throughput for observation patients and enhance communications with patients and their families. OCMTs ensure compliance with protocols, identify and resolve any barriers to treatment or discharge of observation patients, and manage and facilitate expectations and education for patients and family members. Key capabilities represented on the team include clinical care, case management, and utilization management (Figure 2). OCMTs conduct regular rounds of observation patients throughout the day at regular intervals (e.g., every four to six hours) to monitor and update the status of observation patients.
Figure 2: An Observation Care Management Team
Dedicated observation units. A dedicated unit for observation patients serves several purposes. It allows emergency and inpatient units to optimize the use of their space for patients who need higher acuity services. It enables dedicated observation unit staff, such as an OCMT, to focus their care on the specific needs of observation patients. For patients and their family members, it builds understanding and awareness that observation is a standard form of patient status and that the patient is receiving an appropriate level of care for that status along with the other observation patients on the unit.
Contract review. As noted above, commercial health plans have followed CMS’s lead and are closely monitoring assignment of patient status. Commercial health plans may or may not use CMS’s two-midnight rule. In any event, contracts should be reviewed to ensure that the criteria for determining observation status are clearly defined. If they are not, the hospital should negotiate these terms with the health plan and update the contract.
Community partnerships. The COVID-19 pandemic has focused even more attention on inequities in our healthcare system, many of which are driven by social determinants of health that disproportionately affect underprivileged populations. Patients may be held in observation status simply because there is not a safe or supportive environment to which they can be discharged. Partnerships with community organizations that can help improve the patient’s home environment or support the patient at home can make timely discharge a safe and viable option.
Managing observation status requires a focused and consistent effort. Inappropriate assignment of observation status is expensive for patients and hospitals alike and can impede the goal of providing patients with the right care at the right time in the right setting. With new data that enables better benchmarking of observation status, hospital leaders can get a better handle on any issues with observation status assignment in their organization and seek the resources needed to quickly and effectively address these issues. The opportunity can be significant.
Observation Status Protocols
Observation status protocols define criteria indicating that observation status would be appropriate (inclusion criteria) or not appropriate (exclusion criteria). For example, criteria for a chest pain protocol might include:
Observation inclusion criteria
- Negative 1st Troponin (<0.01); Negative EKG
- Chest pain resolves, chest pain intermittent, no EKG changes
- Low (HEART risk score 0 to 3) to moderate risk (HEART risk score 4 to 6)
- Stable vital signs
- No exclusion criteria
Observation exclusion criteria
- Positive troponin (1st draw >0.011)
- Unresolved ischemic chest pain
- EKG changes (consistent with ischemia or high-risk arrhythmia)
- ECG shows evidence of acute myocardial infarction or ischemia pattern
- High risk (HEART risk score 7 or above)
- Stress test or cardiac imaging needed
- Mental illness (patients at risk of self-harm, suicidal, acutely psychotic, inebriation due to alcohol or drugs)







